Question 31#
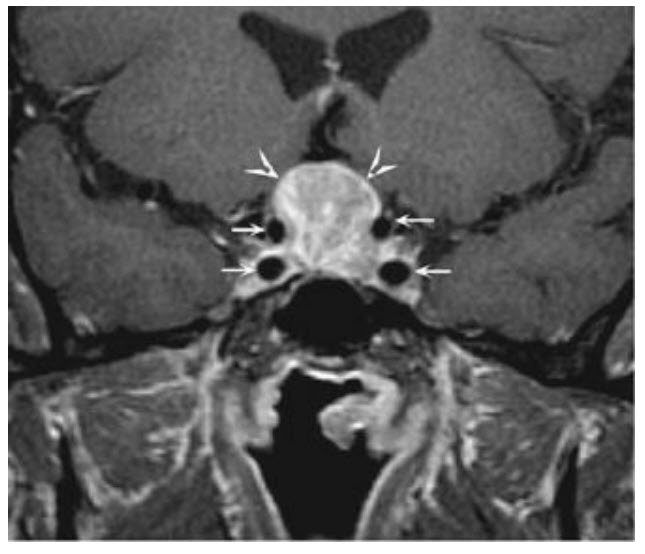
A 36-year-old woman presents with amenorrhea. She has two children aged 8 and 6 years. She took oral contraceptives until her husband had a vasectomy 18 months ago. Since then she has not had a menstrual period. Otherwise she feels well. She takes no medications and exercises regularly but not to excess. She denies headache or galactorrhea. Her physical examination is normal. In particular, visual fields to confrontation are normal. Initial laboratory testing reveals negative pregnancy testing and normal CBC, creatinine, and TSH. Her prolactin level is 225 ng/mL (normal < 20). MRI of the pituitary is shown.
What is the best treatment for this patient’s condition?
A. Transsphenoidal hypophysectomyB. Resume oral contraceptives to reestablish menstrual cycles
C. Somatostatin analogue
D. Dopamine agonist such as cabergoline
E. Observation with yearly prolactin levels and MRI scanning
Correct Answer is D
Comment:
This woman’s amenorrhea is due to her elevated prolactin level. Although certain medications (especially dopamine blockers), hypothyroidism, renal failure, and pregnancy can cause hyperprolactinemia, there is no evidence of these conditions in this patient’s case. Nonpituitary causes rarely elevate the prolactin level above 150. In addition, the MRI shows a macroadenoma (tumor > 1 cm). Prolactin-producing pituitary tumors, even macroadenomas, remain under control of dopamine, which is the physiological prolactin inhibitory factor. In most patients, with dopamine agonist therapy, the prolactin level will normalize, menses will return, and tumor shrinkage will occur. While previously bromocriptine was used, now the longer-acting cabergoline is usually prescribed. Pituitary surgery can usually be avoided, even if visual symptoms are present, with the use of dopamine agonist therapy. Transsphenoidal hypophysectomy is therefore not the best choice. Although some minimally symptomatic patients with microadenomas are treated with hormone replacement therapy, macroadenomas should be shrunken with dopamine agonist therapy. Somatostatin analogues are used to treat certain growth hormone producing tumors, but are not first-line treatment for prolactinomas. Watchful waiting would expose this woman to the risk of osteoporosis from estrogen deficiency as well as tumor growth with possible visual compromise, and would not be the best choice for this young woman.