Question 46#
The patient is a 56-year-old man with hypertension, diabetes, and obesity who was admitted 6 months ago to an outside hospital with a late presentation of an anterior MI. He presented approximately 3 days post MI and underwent cardiac catheterization at 1 week, which showed a total occlusion in the mid-left anterior descending artery (LAD), severe stenoses of the first and second diagonals, and no significant disease in either the right coronary artery (RCA) or left circumflex artery (LCx). The patient was then referred to your hospital for revascularization. The patient, however, failed to show for his appointment and finally presented 8 months later with CP and SOB. Prior to revascularization you order a positron emission tomography (PET) rubidium (Rb)/fluorodeoxyglucose (FDG) using Rubidium82 /F18A (flourine-18–labeled deoxyglucose) to determine the degree of inducible ischemia and viability. The images obtained are in Figure below.
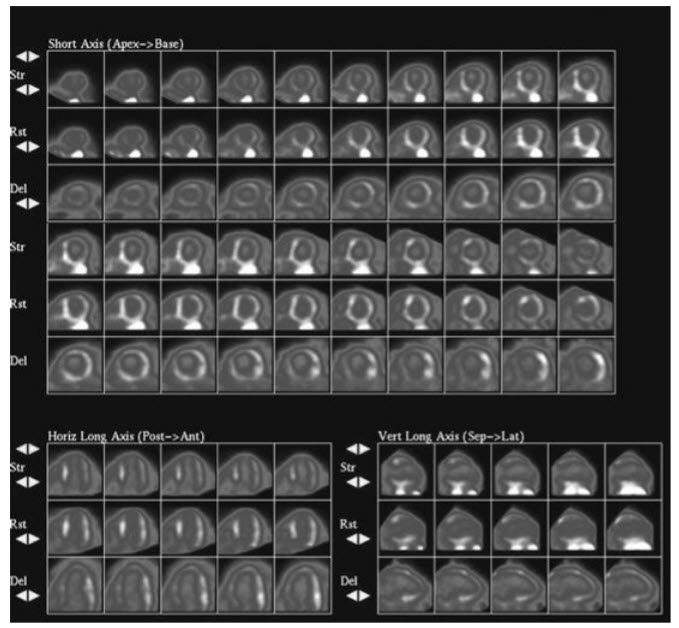
Rubidium/FDG PET scan with the stress images displayed on top, the rest images next, and the delayed metabolic FDG images displayed on the bottom.
The images from the PET scan demonstrate:
A. Scar in the LAD territoryB. Inducible ischemia in the LAD territory
C. Hibernating Myocardium in the LAD territory
D. A combination of inducible ischemia and hibernation in the LAD territory
E. Scar in the RCA territory
Correct Answer is C
Comment:
Hibernating myocardium in the LAD territory. There is a matched defect in the LAD territory seen on the resting and post-stress images involving the apex and four periapical segments as well as the mid-anterior and anteroapical segments. This is consistent with a large LAD territory infarct without any inducible ischemia. The metabolic FDG images show a perfusion/metabolism mismatch with FDG uptake seen in the previously mentioned LAD segments, suggesting a large region of hibernation in the LAD territory without any significant scar. (Note that there is significant gastrointestinal [GI] uptake near the inferior wall.) The degree of hibernation involved 40% of the myocardium (6% for each involved segment except for the apex, which represents 4% of the myocardium). A study by Hachamovitch et al. 1 in 2003 showed that revascularization was superior to medical therapy if the amount of myocardium at risk (ischemic and hibernating) exceeded 20%. Since the above patient demonstrated a large area of hibernating myocardium in the LAD territory, the patient would benefit from revascularization of the LAD territory as well as the diagonals. This patient underwent surgical revascularization of all three vessels.