Question 49#
The patient is a 60-year-old man with hypertension, diabetes (newly diagnosed), and CAD (s/p percutaneous coronary intervention with drugeluting stent in his mid-LAD 5 years ago, and bare metal stent to distal RCA, and a posteroventricular branch 7 years ago). The patient is now sent for symptom evaluation. The patient notes the onset of CPs with exertion while playing squash approximately 2 months ago. The pain occurs only with activity and resolves within a few minutes with rest. He denies other associated symptoms or discomfort at rest. A treadmill nuclear stress test was performed. The patient exercised using a standard Bruce protocol having completed eight metabolic equivalents and reached 98% maximum predicted heart rate (MPHR). There was a normal ST-segment response to stress, and there was no CP with exercise. He did, however, develop new ST depressions in recovery and new atrial fibrillation in recovery, requiring treatment with β-blockers. The scan images are shown in Figure below.
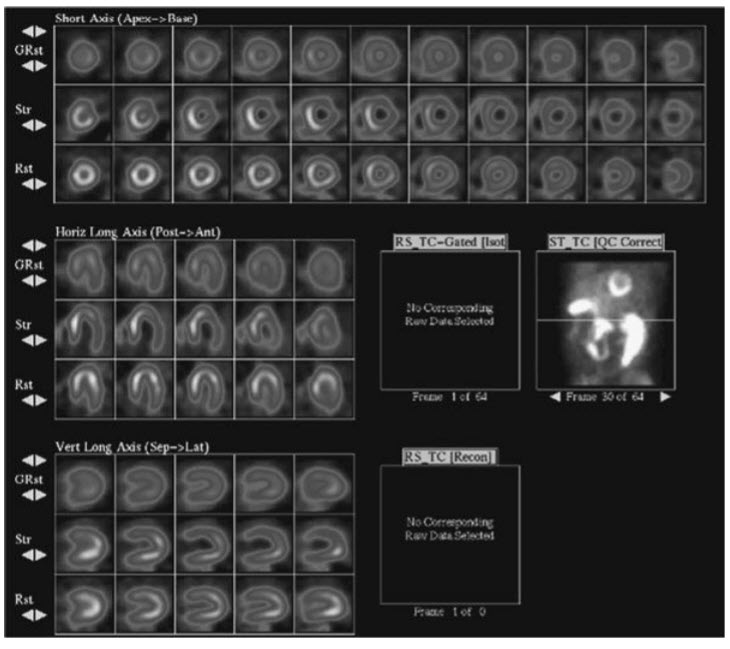
An exercise technetium-99m nuclear stress test with the stress images with the gated images (currently still) on top, the post-stress images next, and the resting images on the bottom.
The appropriate interpretation of this scan is:
A. RCA territory infarctB. LAD territory infarct
C. RCA territory ischemia
D. LAD infarct with peri-infarct ischemia
E. LAD and LCx versus left main ischemia
Correct Answer is E
Comment:
LAD and LCx versus left main ischemia. The resting images demonstrate normal perfusion. Post stress, however, there are significant perfusion defects in the anterior, anterolateral, and inferolateral walls. There is also cavity dilatation, which is consistent with either left main disease or multivessel ischemia. The gated images showed new wall motion abnormalities in the LAD and LCx territories. The presence of stressinduced perfusion defects in multiple vascular territories as well as TID and new wall motion abnormalities on the gated images are all findings associated with high-risk scans. The cardiac catheterization in this patient demonstrated 70% stenosis in the proximal LAD, while the stent in the mid- LAD was patent. There was a large obtuse marginal with a 90% proximal stenosis. There was mild disease in the proximal RCA, and the stents in posterior descending artery and posteroventricular branch were patent.