Question 1#
A 79-year-old female with history of hypertension and right-sided subdural hemorrhage status-post right hemicraniectomy and cranioplasty presented to the emergency department with progressive head and focal right arm twitching concerning for a focal seizure. A head CT was obtained and is shown in the figure below:
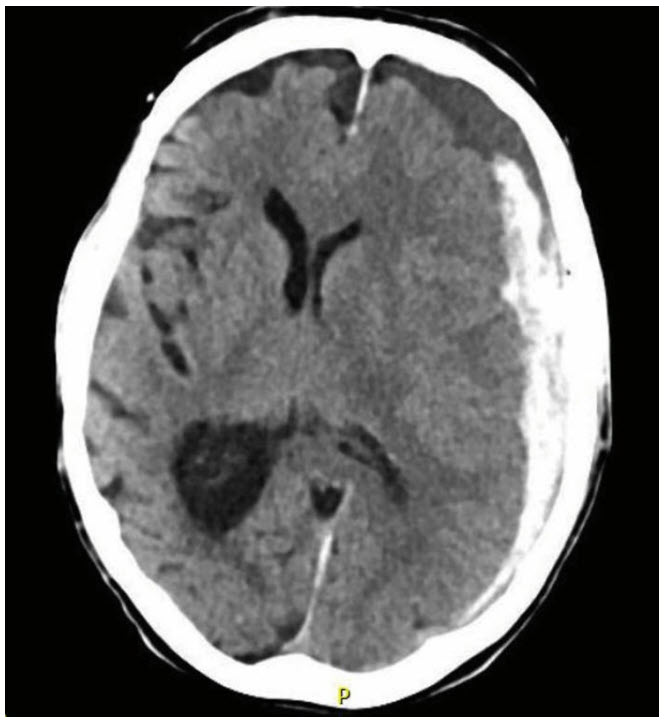
What type of herniation is demonstrated on the head CT and what are the anticipated neurologic findings on examination?
A. Fungating herniation—contralateral > ipsilateral weaknessB. Subfalcine herniation—contralateral > ipsilateral leg weakness
C. Transtentorial (uncal) herniation—contralateral weakness and anisocoria
D. Tonsillar herniation—marked depressed level of consciousness and bulbar dysfunction
Correct Answer is B
Comment:
Correct Answer: B
The head CT above demonstrates an acute on subacute left-sided subdural hemorrhage with left-to-right midline shift and compression of the left lateral ventricle and potential trapping of the right lateral ventricle. The timing of the subdural hemorrhage is based on the density of the blood product. Acute blood appears hyperdense to brain parenchyma. After approximately 3 days the blood product begins to break down and will reach an isodense characteristic compared to brain parenchyma, typically around 10 to 14 days. After 21 days, the blood product becomes hypodense to brain tissue and is similar to cerebrospinal fluid. The herniation demonstrated on this image is subfalcine with left frontal lobe shift under the falx into the right hemisphere. Subfalcine herniation results with cingulate gyrus herniation across the falx and compression of the pericallosal arteries resulting in contralateral (and commonly bilateral) leg weakness. Transtentorial or uncal herniation occurs with the medial temporal lobe and uncus compresses the ipsilateral cerebral peduncle resulting in compression of the ipsilateral third cranial nerve resulting in an enlarged and fixed or sluggishly reactive pupil and contralateral weakness. Tonsillar herniation occurs when there is a pressure within the cerebellum resulting in herniation of the cerebellar tonsil into the foramen magnum and compression of the fourth ventricle resulting in noncommunicating hydrocephalus and obtundation. Fungating herniation occurs when there is a skull defect and herniation of brain tissue outside the cranial vault. All herniation occurs due to a pressure gradient from one compartment (left-right hemisphere, or supra-infratentorial compartment).
References:
- Brant WE, Helms CA. Fundamentals of Diagnostic Radiology. Lippincott Williams & Wilkins; 2007.
- Blumenfeld H. Neuroanatomy Through Clinical Cases. 2nd ed. Sinauer Associates; 2010.