Question 3#
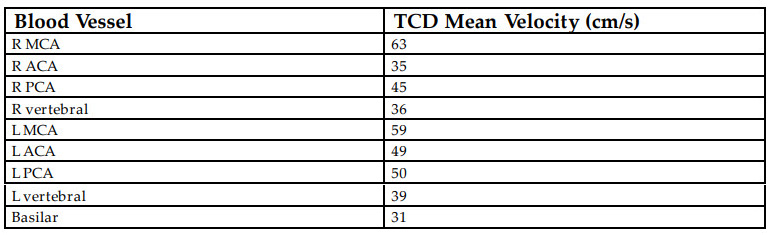
A 55-year-old female with lupus (on hydroxychloroquine) and hypertension was brought to the emergency department for obtundation. She was intubated in the field given agonal respirations. CT angiogram revealed diffuse subarachnoid hemorrhage and an anterior communicating artery aneurysm. The aneurysm was secured with endovascular coiling. On hospital day 8 the patient had worsening of her examination with weakness of the left face, arm, and leg, as well as mild dysarthria. Her transcranial Doppler ultrasound results are shown below. Angiography was done to evaluate for potential cerebral artery vasospasm. Mild-tomoderate right proximal anterior communicating artery vasospasm was found and treated with intra-arterial verapamil resulting in angiographic and clinical improvement of her symptoms.
Which of the comments is true regarding the use of transcranial Doppler ultrasound for cerebral artery vasospasm following aneurysmal subarachnoid hemorrhage?
A. The most reliable blood vessels for evaluating vasospasm via transcranial Doppler ultrasound is the anterior cerebral artery and vertebral arteryB. If there is vasospasm (defined as mean velocity >120 cm/s) present on transcranial Doppler, there will be clinical changes
C. Lindegaard ratio can help evaluate the etiology of elevated mean velocities by comparing the middle cerebral artery and ipsilateral extracranial carotid artery velocities
D. Following intra-aterial treatment with verapamil, transcranial Doppler velocities will typically increase due to hyperemia
Correct Answer is C
Comment:
Correct Answer: C
Transcranial Doppler ultrasound (TCD) is a noninvasive, easily reproducible test that can be used to monitor for cerebral artery vasospasm following aneurysmal subarachnoid hemorrhage. It can be used for other disease evaluation including emboli detection, brain death evaluation, and sickle cell disease. TCD uses low-frequency (2 MHz) pulse Doppler to evaluate velocity of blood flow through the proximal intra- and extracranial arteries. Although a good screening tool, it has limited sensitivity (90%), specificity (70%), and positive predictive value (57%) when compared to digital subtraction angiography. Early studies using TCD evaluated the diameter of blood vessels and the mean velocity. Mean velocities >120 cm/s correlated with decrease in blood vessel diameter by 50%. The patient’s transcranial Doppler ultrasounds are normal despite having angiographic and clinical vasospasm which can be seen given the sensitivity of the testing. More importantly, there are limitations in the ability to TCD to detect vasospasm in major blood vessels other than the middle cerebral and basilar arteries. Although not present here, elevated velocities may not be a sign of vasospasm. At times there can be hyperemia resulting in increased velocities throughout. The advent of the Lindegaard ratio can be used to further evaluate elevation in velocities by comparing the mean velocity in the middle cerebral artery with that of the ipsilateral extracranial internal carotid artery (MEANmca/MEANeica) with ratios of 3 to 6 consistent with mild spasm and >6 moderate spasm while a ratio of <3 meaning there is increased flow throughout the vascular system. Lindegaard ratio >3 and mean velocity >120 cm/s correlated with clinical vasospasm 85% and angiographic vasospasm 83.2%. There are many treatment options for angiographic vasospasm and verapamil works by blocking L-type calcium channels and results in relaxation of smooth muscle. Following treatment with verapamil mean TCD velocities will decrease rather than increase.
References:
- Purykayastha S, Sorond F. Transcranial Doppler ultrasound: technique and application. Semin Neurol. 2012;32:411-420.
- White H, Venkatesh B. Application of transcranial Doppler in the ICU: a review. Intensive Care Med. 2006;32:981-994.
- Kumar G, Shahripour RB, Harrrigan MR. Vasospasm on transcranial Doppler is predictive of delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage: a systematic review and meta-analysis. J Neurosurg. 2016;124:1257-1264.
- Lindegaard KF, Nornes H, Bakke SJ, et al. Cerebral vasospasm diagnosis by means of angiography and blood velocity measurements. Acta Neurochir (Wien). 1989;100:12-24.
- Gonzalez NR, Boscardin WJ, Glenn T, et al. Vasospasm probability index: a combination of transcranial doppler velocities, cerebral blood flow and clinical risk factors to predict cerebral vasospasm after aneurysmal subarachnoid hemorrhage. J Neurosurg. 2007;107:1101- 1112.
- Sayama CM, Jiu JK, Caldwell WT. Update on endovascular therapies for cerebral vasospasm induced by aneurysmal subarachnoid hemorrhage. Neurosurg Focus. 2006;21:E12.