Question 8#
An 88-year-old male with complex coronary disease that includes prior three-vessel coronary artery bypass grafting and prior complete heart block necessitating dual chamber permanent pacemaker implantation presents with substernal chest pain identical in character to his past angina.
His presenting electrocardiogram is:
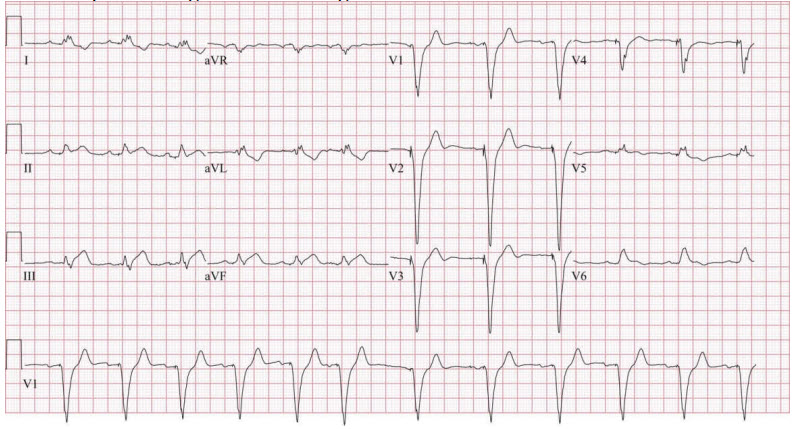
His presenting troponin-T is 0.54 ng/mL (reference <0.03 ng/mL).
Which of the following is the next best step in management?
A. Emergent coronary angiography with the intent to revascularizeB. Urgent (24-48 hours) coronary angiography with the intent to revascularize
C. Noninvasive risk stratification
D. Intravenous nitroglycerin
Correct Answer is A
Comment:
Correct Answer: A
Early diagnosis of an ST elevation myocardial infarction (STEMI) remains key in determining management. Early diagnosis leads to earlier reperfusion which ultimately improves mortality. Diagnosis of STEMI necessitates the presence of new ST elevations in at least two contiguous leads (of ≥2 mm in men ≥40 years, ≥2.5 mm in men <40 years, or ≥1.5 mm in women in leads V2 -V3 and/or ≥1 mm in other contiguous chest leads or limb leads).
The diagnosis of myocardial ischemia and infarction in the presence of conduction disturbances proves more challenging. Ischemic symptoms with a presumed new left bundle branch block (LBBB) or right bundle branch block (RBBB) that is not rate related is associated with adverse prognosis. In patients with an LBBB, ST segment elevation ≥1 mm concordant with the QRS complex in any lead may be an indicator of acute myocardial ischemia. Similar criteria can be used to diagnose acute myocardial infarction in the presence of right ventricular pacing as demonstrated in this patient’s electrocardiogram. Because of the concordant QRS-ST changes apparent in the inferior leads of this patient’s electrocardiogram, angiography should be pursued.
References:
- Thygesen K, Alpert JS, Jaffe AS, et al; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth universal definition of myocardial infarction (2018). Circulation. 2018;138(20):e618-e651.
- Wang TY, Nallamothu BK, Krumholz HM, et al. Association of door-in to door-out time with reperfusion delays and outcomes among patients transferred for primary percutaneous coronary intervention. JAMA. 2011;305(24):2540-2547.