Question 10#
What is true regarding the evaluation ofblunt abdominal trauma?
A. Patients with abdominal wall rigidity and negative abdominal CT should undergo diagnostic peritoneal lavage (DPL) to rule out small bowel injuryB. If FAST examination is negative in a hemodynamically unstable patient then DPL is indicated to rule out abdominal bleeding
C. FAST examination cannot detect intraperitoneal fluid if the total volume is < 1000 mL
D. Bowel injury can be ruled out in hemodynamically stable patients with abdominal CT scanning
Correct Answer is B
Comment:
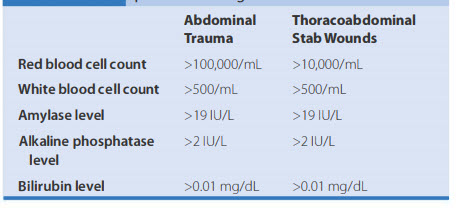
The presence of abdominal rigidity and hemodynamic compromise is an undisputed indication for prompt surgical exploration. Blunt abdominal trauma is evaluated initially by FAST examination in most major trauma centers, and this has largely supplanted diagnostic peritoneal lavage (DPL). FAST is not 100% sensitive, however, so diagnostic peritoneal aspiration is warranted in hemodynamically unstable patients without a defined source of blood loss to rule out abdominal hemorrhage. This method is exquisitely sensitive for detecting intraperitoneal fluid of > 250 mL. Patients with fluid on FAST examination, considered a "positive FAST;' who do not have immediate indications for laparotomy and are hemodynamically stable undergo CT scanning to quantify their injuries. CT also is indicated for hemodynamically stable patients for whom the physical examination is unreliable. Despite the increasing diagnostic accuracy of multidetector CT scanners, identification of intestinal injuries remains a limitation. Patients with free intra-abdominal fluid without solid organ injury are closely monitored for evolving signs of peritonitis; if patients have a significant closed head injury or cannot be serially examined, DPL should be performed to exclude bowel injury. After placement of the catheter, a 10-mL syringe is connected and the abdominal contents aspirated (termed a diagnostic peritoneal aspiration). The aspirate is considered to show positive findings if > 10 mL of blood is aspirated. If < 10 mL is withdrawn, a liter of normal saline is instilled. The effluent is withdrawn via siphoning and sent to the laboratory for red blood cell (RBC) count, white blood cell (WBC) count, and determination of amylase, bilirubin, and alkaline phosphatase levels. See Table below for values representing positive findings.
Criteria for "positive" finding on diagnostic peritoneal lavage: